So, I was really reading a lot in the previous thread "Changing ART Without Genotype Available in the Setting of Cardiac and Renal Comorbidities"; I found myself in clinic the other day meeting a new patient - inherited from another practice within our same health system. Unfortunately, there was very little chart data to work with. The previous provider seemed to favor shorthand notes in the EMR, and from what I can tell, even they had inherited the patient without a full history.
This patient has had developing resistance over time, largely due to changes in care, living arrangements, and challenges with adherence related to behavioral health. Generally, I'm not a huge fan of running GenoArchives unless necessary - but in this case, I did. And the number of RAMs... woooweee.
Dr. Gallant's point in a previous thread - "if it ain't broke..." - really resonates. I typically like to optimize regimens when possible (reduce DDIs for aging patients, simplify to STRs, switch to an INSTI-based regimen if appropriate, minimize pill burden, etc.). Well, my game was a little off here.
The patient was initially on ABC/3TC/DTG + DRV/c. I decided to switch him to B/F/TAF + DRV/c for the reasons above. However, once the archive came back, it showed pan-resistance to INSTIs and most NRTIs/NNRTIs - but thankfully, no PI resistance.
To note: the patient was fully suppressed at the time of my first visit (it was an NPV), although there were prior fluctuations in VL (mostly undetectable as per records in the chart from 2017, but at least 3-4 blips of low level viremia of under 1000 copies). We've really emphasized adherence - and to his credit, he seems to like me, the clinic, and the team here, and is now more engaged with his medical case manager.
That being said... I now had this new (unlucky) data to contend with. I brought him back in and switched the regimen to DOR + DRV/c.
The whole point of this post:
Does anyone have patients on this regimen? While it's two active agents, it's not my go-to choice - but alas, here we are.
I'd love any feedback. (Not looking at LEN + oral at this time; the only patients I have on LEN are on LEN/CAB/RPV.)
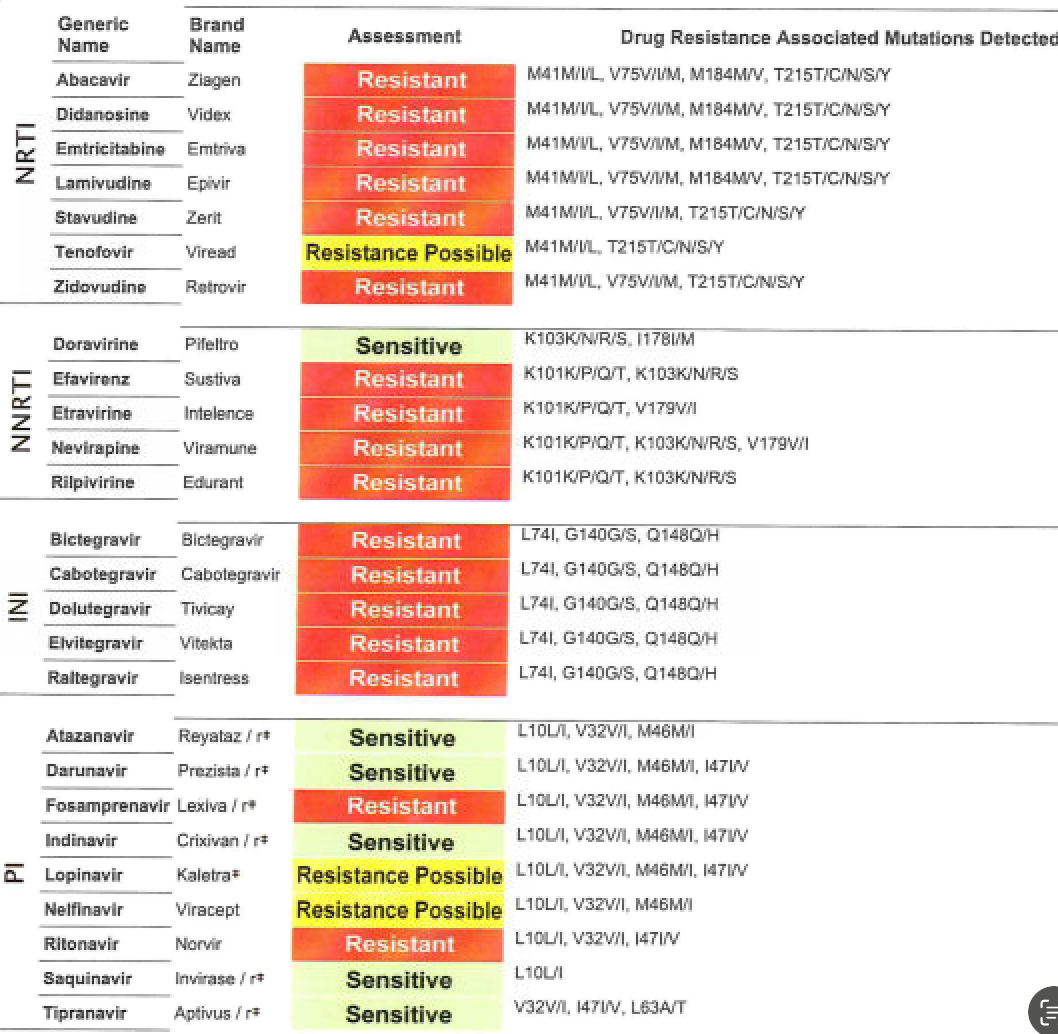
See Archive:
------------------------------
Ashwin Gupta
PA
------------------------------